|
|
|
|
|
|
|
|
|
|
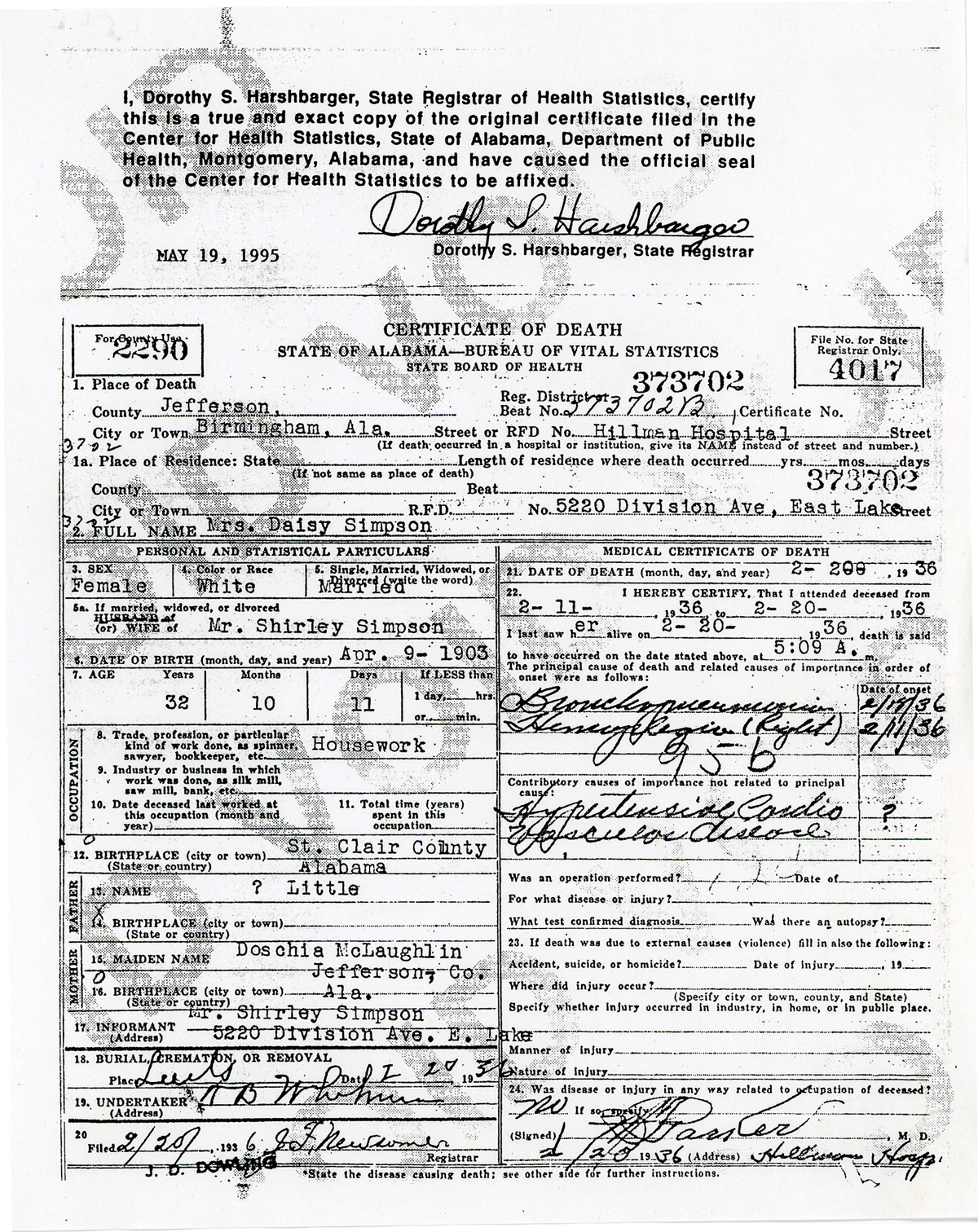
Daisy
Little Simpson's Death |
|||||
|
Daisy Little died tragically at age 32 on February 20th, 1936. She left behind her husband and six children ranging in age from 2 months to 12 years. Little is known about the circumstances surrounding her untimely death. Family discussions include that she may have died from complications arising from the birth of her youngest child, Andrew Lewis or that she died from malnutrition as it is thought that her husband Shirley did not provide for her or his family. It is known that upon her death, Shirley gave up his children dispersing them among Daisy's sisters. Reviewing Daisy's Death certificate, it appears that she died of pneumonia and the complications of a stroke which was likely the result of chronic hypertension (high blood pressure) and childbirth. The Death Certificate indicates that she was admitted to Hillman Hospital on February 11, 1936 paralyzed on the right side of her body and that she suffered from high blood pressure. The primary causes of death shown are Bronchopneumonia and hemiplegia (paralysis on one side of the body commonly resulting from a stoke). It is likely that the combination of her high blood pressure and her recent childbirth led to a stroke as evidenced by her paralysis. She then likely contracted pneumonia while in the hospital and died. The current average age of individuals suffering a stroke in the United States is 70. So, it is rare that Daisy had a stroke at the age of 32. Additionally, the incidence of stroke brought on by pregnancy or childbirth is 8 in 100,000, also very rare. However, according to blackhealth.com, the risk of stroke during the six weeks after childbirth is 9 to 28 times higher than that for non-pregnant or post-partum women. Daisy gave birth 7 weeks before her apparent stroke.
Detailed
Medical Explanation Paralysis is a common feature of stroke, often on one side of the body (hemiplegia). The paralysis or weakness may affect only the face, an arm, or a leg or may affect one entire side of the body and face. A person who suffers a stroke in the left hemisphere of the brain will show right-sided paralysis or paresis. Conversely, a person with a stroke in the right hemisphere of the brain will show deficits on the left side of the body. Stroke
and Childbirth A study sponsored by the NINDS showed that the risk of stroke during pregnancy is greatest in the post-partum period – the 6 weeks following childbirth. The risk of ischemic stroke after pregnancy is about nine times higher and the risk of hemorrhagic stroke is more than 28 times higher for post-partum women than for women who are not pregnant or post-partum. The cause is unknown. Hemiplegia Hypertensive
Cardiovascular Disease or HCVD Thus, hypertensive heart disease is a term applied generally to heart diseases, such as LVH, coronary artery disease, cardiac arrhythmias, and CHF, caused by direct or indirect effects of elevated BP. [Cardiac
arrhythmias,one of] the [] various cardiac effects of hypertension []
is described [below]: Cardiac arrhythmias commonly observed in patients with hypertension include atrial fibrillation, premature ventricular contractions, and ventricular tachycardia. The risk of sudden cardiac death is increased. Various mechanisms thought to play a part in [] arrhythmias include altered cellular structure and metabolism, inhomogeneity of the myocardium, poor perfusion, myocardial fibrosis, and fluctuation in afterload. All of these may lead to an increased risk of ventricular tachyarrhythmias. Atrial fibrillation (paroxysmal, chronic recurrent, or chronic persistent) is observed frequently in patients with hypertension. In fact, elevated BP is the most common cause of atrial fibrillation in the Western hemisphere. In one study, nearly 50% of patients with atrial fibrillation had hypertension. Although the exact etiology is not known, left atrial structural abnormalities, associated coronary artery disease, and LVH have been suggested as possible contributing factors. The development of atrial fibrillation can cause decompensation of systolic and, more importantly, diastolic dysfunction, owing to loss of atrial kick, and it also increases the risk of thromboembolic complications, most notably stroke. Cerebral
involvement in hypertensive cardiovascular disease |
|||||
|
|
|
|
|
|
|
Copyright
© 2006-8 Old Joes Inc. All Rights Reserved. Designated trademarks
and brands are the property of their respective owners.
|